
The Persistent Echo of Alarms: Understanding and Navigating Diabetes Distress
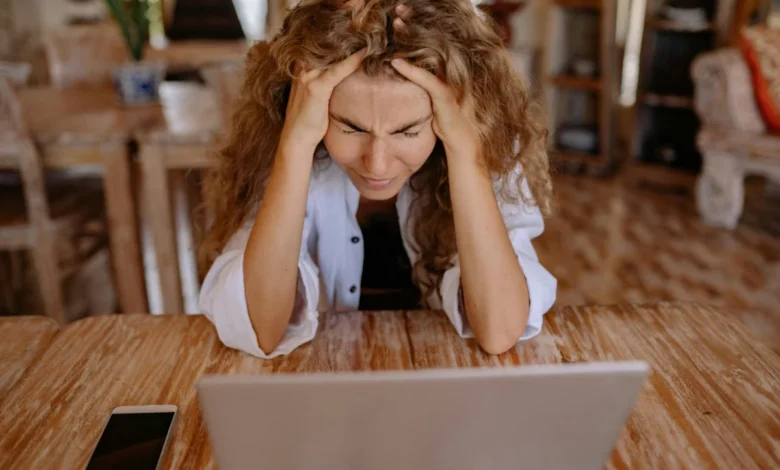
The insistent, piercing sound of a continuous glucose monitor (CGM) alarm, punctuated by the involuntary expletive that follows, is a visceral signal for many living with diabetes. It marks not just a deviation in blood glucose levels, but often the insidious onset of what healthcare professionals term "diabetes distress." This phenomenon, while distinct from clinical depression or burnout, represents a significant emotional burden that accompanies the daily, relentless task of managing a chronic condition. For individuals like the author of the original anecdotal account, these alarms are the first indication that the intricate dance of diabetes management is leading them into a state of emotional turmoil.
The evolution of diabetes management over the past four decades has been nothing short of revolutionary. From the rudimentary urine testing and rigid exchange diets of the pre-digital era, to the sophisticated automated insulin delivery systems and real-time glucose monitoring available today, the tools at the disposal of individuals with diabetes have dramatically advanced. Yet, despite these technological leaps, the fundamental challenge of maintaining stable blood glucose levels remains, and for many, the emotional toll has not diminished. The author reflects on a time when their mother meticulously mixed two types of insulin in a single syringe, a stark contrast to the precision offered by modern pens and pumps. This historical perspective underscores the progress made, but also highlights the enduring complexity and inherent difficulty of living with diabetes.
The frustration associated with diabetes distress often stems from a perceived disconnect between effort and outcome. Individuals meticulously follow prescribed routines: counting carbohydrates with precision, calculating and administering insulin doses, diligently monitoring glucose trends, and making frequent micro-adjustments. These actions, honed over years, even decades, of living with the condition, are intended to yield predictable results. However, the reality of diabetes management is frequently characterized by an unsettling unpredictability.
One week, a person might find that the same foods they have consumed without issue for months suddenly trigger a dramatic spike in blood glucose levels. Despite replicating the exact carbohydrate count, bolus timing, and pre-meal glucose levels, the CGM displays an upward trend, culminating in a high glucose alarm. This scenario, characterized by the author as "everything I eat sends my numbers skyrocketing," is a common trigger for distress. The feeling of losing control, of one’s body not responding as expected, can be deeply demoralizing.
Conversely, the following week, the opposite scenario might unfold. The same meticulous routines that led to high numbers the week prior could now result in persistently low glucose levels, prompting a different set of alarms and anxieties. This oscillation between hyperglycemia and hypoglycemia, despite consistent management strategies, underscores the multifaceted nature of diabetes control. Factors such as hormonal fluctuations, stress levels, sleep quality, illness, travel, and even environmental changes like weather can significantly impact glucose metabolism, often in ways that are not immediately apparent or controllable.
When these unpredictable swings become frequent, and interventions seem ineffective, the cumulative emotional weight of diabetes management can become overwhelming. The constant cognitive load of decision-making, the intricate calculations, the unwavering vigilance required, and the gnawing feeling that despite all efforts, diabetes still holds sway, contribute to the development of diabetes distress. This emotional burden is not a sign of personal failing but a natural consequence of managing a condition that demands constant attention and adaptation.
Defining Diabetes Distress
Diabetes distress, as defined by leading diabetes organizations, is the emotional strain and psychological burden that arises from the daily demands of living with and managing diabetes. It is important to distinguish it from clinical depression or diabetes burnout, although it can certainly coexist with or lead to these conditions. Burnout, for instance, often manifests as a feeling of exhaustion and a loss of motivation to continue managing the condition. Depression, on the other hand, is a clinical mood disorder characterized by persistent sadness, loss of interest, and other debilitating symptoms.
Diabetes distress, however, is more specifically tied to the emotional responses elicited by the practicalities of diabetes management. It can manifest as a spectrum of negative emotions, including frustration, guilt, anger, anxiety, and profound exhaustion. For some, it is the overwhelming feeling of being bombarded by constant data from monitoring devices, each number a potential cause for concern. For others, it is the sense that every meal, every activity, and every decision is a potential battleground where diabetes, the unseen adversary, might emerge victorious. The author’s description of CGM alarms and subsequent expletives perfectly encapsulates this feeling of an ongoing, often frustrating, struggle.
The Pervasiveness of Diabetes Distress
Research consistently indicates that a significant proportion of individuals living with diabetes experience diabetes distress at various points in their lives. A study published in Diabetes Care found that over 30% of adults with type 1 and type 2 diabetes reported experiencing diabetes distress. This prevalence underscores that such feelings are not isolated incidents but a common and often expected aspect of the diabetes journey. Managing diabetes requires hundreds, if not thousands, of micro-decisions daily. These range from deciding what to eat, how much insulin to take, when to exercise, and how to respond to unexpected physiological changes. The inherent unpredictability of these outcomes, coupled with the constant need for vigilance, makes the process inherently taxing.
The cyclical nature of diabetes management means that weeks of relatively stable glucose control can be abruptly disrupted. A stressful work deadline, a sleepless night, a minor illness, or even a change in routine due to travel can throw the delicate balance off-kilter. When these disruptions occur, it is easy for individuals to fall into the trap of self-blame, believing they have somehow failed in their management efforts. However, diabetes is not a simple mathematical equation with a guaranteed solution. It is a complex biological system influenced by a myriad of internal and external variables, many of which are beyond immediate control.
For individuals who identify as perfectionists, this lack of guaranteed control can be particularly challenging. The desire to achieve perfect blood glucose readings and flawless management can clash with the inherent variability of the condition. This disconnect between the aspiration for perfection and the reality of diabetes can be a significant source of distress. The understanding that perfection is an unattainable goal in diabetes management is a crucial, albeit difficult, realization.
Strategies for Mitigating Diabetes Distress
Recognizing diabetes distress as a normal and expected part of living with the condition is the first step toward managing it effectively. Rather than pushing harder or attempting to "fix" every deviation immediately, a more beneficial approach often involves pausing and resetting. This can take many forms, tailored to individual needs and preferences.
One common and effective strategy is to acknowledge and validate the feelings of frustration or overwhelm. Simply recognizing that these emotions are a response to a challenging situation, rather than a personal failing, can alleviate some of the self-imposed pressure. This self-compassion is crucial. It involves treating oneself with the same kindness and understanding that one would offer to a friend facing similar difficulties.
Taking breaks from intensive monitoring can also be beneficial. This doesn’t mean abandoning management altogether, but rather consciously stepping away from the constant data stream for short periods. This might involve putting away the CGM reader for a few hours, focusing on other activities, or engaging in mindfulness exercises to bring the focus back to the present moment without the pressure of glucose numbers.
Seeking support is another vital component of managing diabetes distress. This can involve connecting with other individuals who live with diabetes through support groups, online forums, or peer mentoring programs. Sharing experiences and realizing that one is not alone in these struggles can be incredibly validating and empowering. Healthcare providers, including endocrinologists, certified diabetes educators, and mental health professionals specializing in chronic illness, also play a critical role. They can offer practical strategies, emotional support, and, when necessary, clinical interventions for managing distress.
Adjusting management strategies in collaboration with healthcare providers is also important. When certain approaches consistently lead to frustration or seem ineffective, it signals a need for re-evaluation. This might involve exploring different insulin regimens, dietary approaches, or exercise plans. The key is to approach these adjustments not as a sign of failure, but as a proactive step towards finding a more sustainable and less distressing management plan.
Ultimately, the goal is to foster a more balanced and compassionate approach to diabetes management. It is about recognizing that while diabetes requires constant attention, it should not consume one’s entire emotional and psychological well-being. The alarms from a CGM, while often irritating, can serve as a reminder to pause, breathe, and re-evaluate the approach to self-care. Managing diabetes is not about achieving perfect performance every moment of every day; it is a long-term journey that requires resilience, adaptability, and a significant amount of self-kindness. By understanding and addressing diabetes distress, individuals can navigate the complexities of their condition with greater emotional strength and well-being.





{kind=link}