
Mastering the Art of Inquiry How Intentional Conversations with Young Children Foster Long-Term Cognitive and Social Development
The developmental trajectory of a child is often shaped not by the answers they receive, but by the quality of the dialogue that follows their questions. In the recently released pedagogical guide, Rich Talk With Young Children, Dr. Rebecca Rolland, a faculty member at the Harvard Graduate School of Education and a speech-language pathologist, outlines a transformative framework for early childhood communication. This methodology, centered on "rich talk," posits that the frequent "why" and "how" questions posed by children aged two to eight are not merely repetitive queries but critical neurological windows for learning. When educators and caregivers engage deeply with these inquiries rather than offering dismissive or one-word responses, they activate a complex web of cognitive and emotional benefits that can define a child’s academic and social success for years to reach.
The Science of Conversational Turns and Brain Development
The concept of "Rich Talk" is grounded in the "serve and return" model of interaction, a concept championed by the Center on the Developing Child at Harvard University. In this model, a child "serves" a question or a gesture, and the adult "returns" it with an appropriate, stimulating response. Research indicates that the number of "conversational turns"—the back-and-forth exchanges between a child and an adult—is a more accurate predictor of future brain structure and language skills than the total number of words a child hears.
A landmark study published in the journal Psychological Science demonstrated that children who engaged in more frequent conversational turns showed greater activation in the Broca’s area, a region of the brain linked to speech production and language processing. This activation occurred regardless of the family’s socioeconomic status or the sheer volume of words spoken in the household. By leaning into "why" and "how" questions, adults facilitate these high-value conversational turns, effectively "wiring" the child’s brain for complex thought and emotional regulation.

Ten Strategies for Navigating the Inquiry Phase
To maximize the impact of these interactions, Dr. Rolland and early childhood experts suggest ten specific strategies designed to turn a simple question into a robust learning opportunity. These strategies move beyond the dissemination of facts and toward the cultivation of a growth mindset.
- Validate the Inquiry Immediately: Acknowledging the importance of the question—even if the answer is not immediately known—signals to the child that their curiosity is a valuable asset. This builds the confidence necessary for lifelong learning.
- Practice the Five-Second Rule: Before answering, adults are encouraged to wait five seconds. This "wait time" allows the child to process their own thoughts and perhaps even attempt to answer the question themselves, fostering independent thinking.
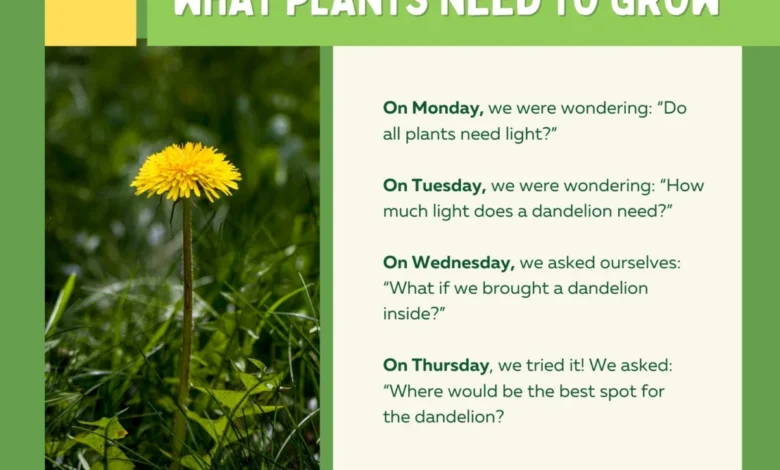
- Encourage "Hypothesis Testing": When a child asks "why is the sky blue?" an effective strategy is to ask, "What do you think makes it blue?" This encourages the child to use their current knowledge to form a hypothesis, a fundamental pillar of the scientific method.
- Use Precise and Varied Vocabulary: Rather than simplifying language to a basic level, adults should use specific terms. If a child asks how a plant grows, using words like "photosynthesis" or "nutrients" in context helps expand their lexicon.
- Connect Questions to Personal Experience: Relate the "how" or "why" to something the child has previously seen or done. This creates "associative bridges" in the brain, making the new information easier to retain.
- Model the Search for Knowledge: If an adult does not know the answer, they should say so and then demonstrate how to find it. This models resourcefulness and shows that learning is a continuous process even for adults.
- Maintain Physical Proximity and Eye Contact: Lowering oneself to the child’s eye level creates a sense of safety and focused attention, which lowers the child’s cortisol levels and makes them more receptive to learning.
- Avoid the "Dead-End" Answer: A "dead-end" answer is one that terminates the conversation, such as "Because that’s just how it is." Instead, use "open-loop" responses that invite further questioning.
- Acknowledge the Emotional Underpinning: Sometimes "why" questions are rooted in anxiety or fear (e.g., "Why is it raining so hard?"). Addressing the emotion behind the question is as important as answering the factual query.
- Scaffold the Complexity: Provide just enough information to satisfy the current curiosity while leaving room for the child to take the next logical step in their reasoning.
A Chronology of Early Childhood Language Milestones
Understanding the evolution of children’s questioning provides essential context for why "Rich Talk" is effective. The progression of inquiry is a reliable marker of cognitive maturation:
- 18–24 Months: The "What" Phase. Children begin labeling their world. Questions are primarily used to identify objects and people, building the foundational vocabulary required for later inquiry.
- 2–3 Years: The Emergence of "Why." This marks a shift from labeling the world to understanding the relationships within it. At this stage, "why" is often used to keep a conversation going as much as it is to seek information.
- 4–5 Years: The "How" and "Why" Sophistication. Children begin to understand cause and effect. Their questions become more targeted and are used to solve problems or understand social norms and rules.
- 6–8 Years: The Abstract Inquiry. Questions move from the immediate physical environment to abstract concepts, moral dilemmas, and complex systems (e.g., "Why do people have different beliefs?").
By recognizing these stages, educators can tailor their "Rich Talk" to meet the child at their current developmental level, ensuring the dialogue is neither too simple nor overwhelmingly complex.
Educational and Institutional Responses
The shift toward intentional conversation has gained significant traction within the global educational community. The National Association for the Education of Young Children (NAEYC) has increasingly emphasized "intentional teaching," which mirrors the principles of Rich Talk. Educators are being trained to move away from rote memorization and toward "inquiry-based learning," where the curriculum is driven by the questions children ask.
In recent surveys of early childhood professionals, over 85% of respondents indicated that the ability to facilitate high-quality classroom discourse was "highly critical" for student readiness in kindergarten. Furthermore, school districts implementing "Rich Talk" frameworks have reported measurable improvements in social-emotional literacy. When children feel heard and their questions are treated with respect, they demonstrate higher levels of empathy and a greater ability to resolve conflicts through verbal communication rather than physical frustration.
Broader Implications and Long-Term Impact
The implications of adopting a "Rich Talk" model extend far beyond the preschool classroom. In an era dominated by digital interfaces and passive screen time, the art of face-to-face, nuanced conversation is becoming a rare and valuable skill. Children who are raised in environments where "why" and "how" questions are explored rather than suppressed are better equipped for the demands of the 21st-century workforce, which prizes critical thinking, collaboration, and complex problem-solving.
Data from longitudinal studies suggest that early linguistic stimulation is a key factor in closing the "achievement gap." The famous 1995 study by Hart and Risley highlighted a "30 million word gap" between children from different socioeconomic backgrounds, but modern analysis suggests the quality and interactive nature of those words are even more impactful than the quantity. Programs that train parents in "Rich Talk" techniques have shown that these interventions can significantly mitigate the effects of economic disadvantage on a child’s cognitive development.
Ultimately, the goal of rich, intentional conversation is to foster a sense of agency in the child. When a child learns that their questions have the power to unlock new worlds of information, they stop being passive recipients of data and start becoming active participants in their own education. As Dr. Rebecca Rolland’s work suggests, the simple act of taking a child’s question seriously is perhaps the most profound educational tool available to any adult. By investing time in these "why" and "how" moments, society is not just teaching children facts; it is teaching them how to think, how to relate to others, and how to navigate an increasingly complex world with curiosity and confidence.






{kind=link}